Article Under Review
This article is undergoing editorial and medical review. We regularly update content as part of our commitment to providing patient-centered, accurate, evidence-based information.
Overview
Not every donation after death happens after brain death. When a patient cannot recover but does not meet the rules for brain death, donation can still happen after the heart stops. This path is called donation after cardiac death, or DCD. It starts with a family decision to withdraw life support. Donation follows once the heart has stopped on its own.
DCD has grown a lot over the past two decades. New ways of caring for donor organs keep them healthy enough to use, even after the heart stops. Many families find this path gives them a way to honor a loved one when no other care can help.
What is donation after cardiac death?
Not all donations happen after brain death. When someone's heart stops and physicians determine it cannot be restarted, families can choose to allow organ donation. This process, called donation after cardiac death (DCD), is becoming more common and offers another path to give the gift of life.
Key aspects of donation after cardiac death:
- Different from brain death. The heart itself has failed, not the brain
- Controlled process. Life support is withdrawn in a planned, organized way
- Time-sensitive. Organs must be recovered quickly after death is declared
- Growing option. More hospitals now offer DCD as families want more donation choices
- Helps waiting list. Expands the donor pool for patients on transplant waiting lists
What is donation after cardiac death?
Donation after cardiac death (DCD) means the person's heart has stopped beating and cannot be restarted. Unlike brain death, where the brain is dead but the heart still pumps with machine support, in DCD the heart itself has failed. The heart cannot be revived no matter what treatment is attempted.
When cardiac death occurs
Cardiac death happens in several situations:
- Massive heart attack. The heart muscle is too damaged to recover
- Chest injuries. Trauma that prevents the heart from functioning
- End-stage heart failure. All treatment options have been exhausted; recovery is not possible
- Heart failure in other conditions. The brain may still function, but the heart will not work
- Medical determination. Physicians determine restarting the heart is not medically possible
If the family chooses donation, organs can still be recovered after cardiac death. Organs no longer receive oxygen-rich blood, creating a different donation path that serves patients on the waiting list.
How is this different?
The fundamental difference is in the sequence of events. In brain death donation, the brain is dead but the heart is still beating. In cardiac death donation, the heart has stopped but the brain may still be functioning.
Brain death donation process:
- Brain is dead (confirmed by testing)
- Heart continues beating with machine support
- Life support maintains organs for transplant
- Death is declared based on neurological criteria
- Donation happens while life support is ongoing
In DCD, the sequence is different and requires a different type of decision. The family chooses to stop life support and allow natural death. Once the heart stops and death is declared by a physician, donation becomes possible.
The brain may still be functioning when this decision is made, which differs from brain death cases where the brain has already been declared dead.
How the process works
Families considering DCD need to understand the full sequence of what will happen and when. This process is very different from brain death donation because it begins with a decision about whether to continue life support. The medical team will be clear about what to expect.
Withdrawal of life support
When medical treatment is no longer helping the person recover and the prognosis is poor, the family and medical team may discuss withdrawing the ventilator or stopping medications that are not extending meaningful life. This happens whether or not donation is being considered. If the family is interested in donation, this conversation includes specific information about the donation process:
- The person will be moved to an operating room
- Life support will be withdrawn
- When the heart stops, death will be declared
- Organ recovery will happen immediately after
Families understand that stopping life support will lead to death regardless of donation. The timeline doesn't change significantly—donation doesn't prolong dying.
The waiting period
After consent for donation is obtained, there's often a waiting period. This wait allows time to find recipients and prepare the surgical team.
The person remains on life support during this time. For families, this waiting can feel anxious, but the medical team keeps you informed about progress.
Which organs can be donated?
After cardiac death, organs may still be viable depending on the person's health and how quickly circulation is restored. Advances in preservation technology have expanded which organs can be recovered from DCD donors.
Organs that may be recovered from DCD donors include:
- Kidneys. Most commonly recovered; can function well even with some warm ischemia time
- Liver. May be recovered, especially with newer preservation techniques like EVHP
- Heart. Increasingly recovered from DCD donors using advanced perfusion and resuscitation techniques to assess and preserve heart function for transplantation.
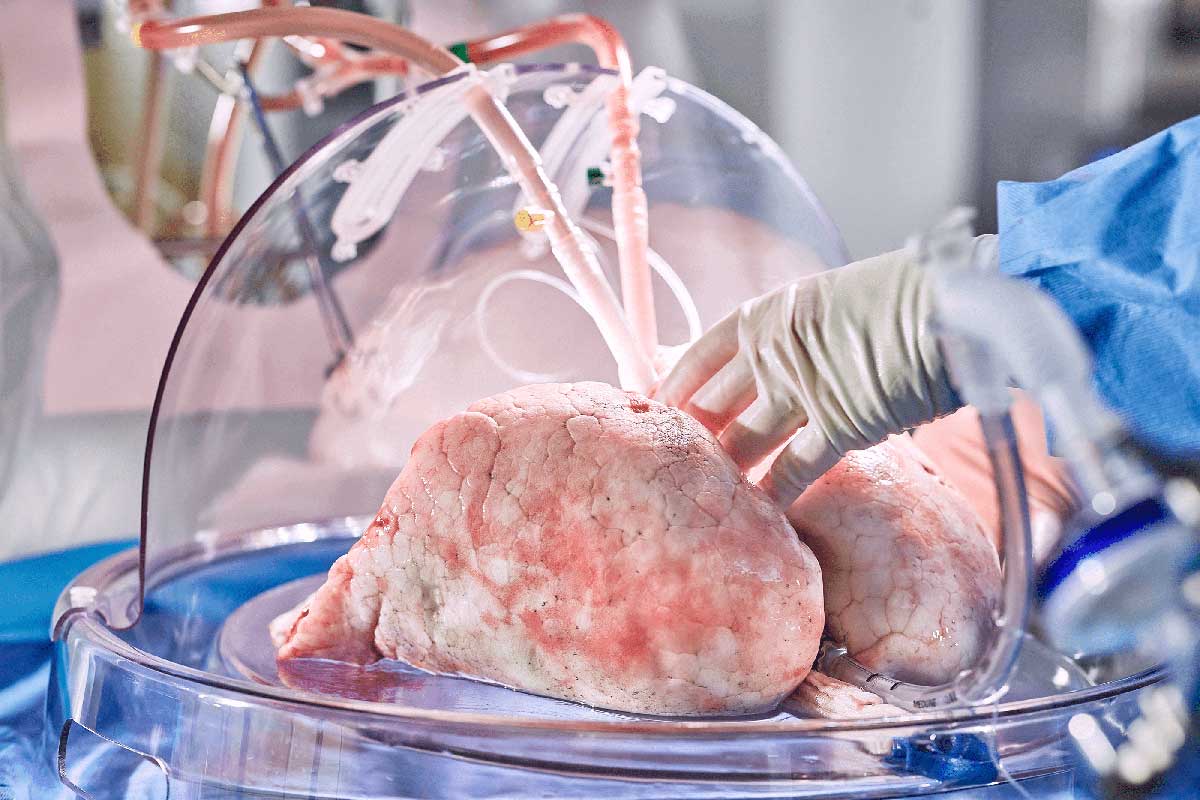
- Lung. Increasingly recovered from DCD donors using ex vivo lung perfusion (EVLP) to assess and recondition them
- Pancreas. Can sometimes be used for transplant; timing is more critical
Tissues may also be recovered—corneas, skin, bone, and connective tissue. Tissue recovery doesn't require the same timing as organs, so tissues can be recovered even if organs aren't viable.
The medical team evaluates which organs are suitable based on the person's condition and medical history. Timing is critical in DCD because organs must be recovered quickly once the heart stops.
Unlike brain death donation where organs receive oxygen-rich blood continuously, DCD organs lose that blood supply immediately when the heart stops. This limits how long they remain viable for transplant.
Questions families ask
Families often have specific concerns about the donation process after cardiac death:
- "Does my family have to be there?" Some families want to be present; others prefer to say goodbye beforehand. Both are valid choices that medical teams accommodate.
- "Is this the same as letting them die?" If life support cannot help recovery, withdrawing it allows natural death. Donation happens after that death. Death is coming regardless—donation gives your loved one's passing a final purpose.
- "How long will organs be usable?" DCD organs have a narrow window. Once the heart stops, organs have limited time before lack of oxygen causes damage. The surgical team works rapidly, usually within 30 minutes.
- "Does organ recovery happen immediately?" Physicians wait a few minutes to confirm no spontaneous heartbeat. Then organ recovery begins in the operating room within an hour.
- "What if the heart doesn't stop quickly?" Occasionally the heart continues beating longer than expected. After an agreed-upon period, if the heart hasn't stopped, natural death occurs and donation may proceed as tissue donation only or may not happen. Families are informed of this possibility beforehand.
Additional Detailed Information
Additional Information
DCD protocols and consent
DCD has specific consent requirements because the family is authorizing withdrawal of life support with the knowledge that donation will follow. The informed consent process requires clear discussion of what will happen and when. Families must understand that the sequence is: (1) decision to withdraw support, (2) withdrawal occurs, (3) death is pronounced, (4) donation happens. There must be clear separation between the team managing the person's care and the transplant team—no conflict of interest is permitted.
Warm ischemia time in DCD
Warm ischemia time (WIT) is the period when the heart has stopped and organs are without oxygen-rich blood. This causes cellular damage. DCD organs experience significant warm ischemia during the period after heart stoppage and before organ perfusion is restored. This is why DCD organs generally have shorter preservation windows and more restrictions on which recipients can receive them. Newer techniques like ex vivo perfusion (EVHP for livers, EVPM for lungs) allow organs to be perfused with preservation solution outside the body, extending preservation time and improving outcomes for some organs.
DCD donor expansion and ethics
DCD protocols have expanded from uncontrolled (unexpected cardiac arrests) to controlled (planned withdrawal of life support) donations. Controlled DCD comprises most current DCD donations. This expansion has raised important ethical discussions about ensuring no conflict of interest and that withdrawal of support decisions are made independently of donation considerations. Strict protocols and oversight prevent these concerns, but they remain important ethical guardrails for the field.
Written By:

Transplants.org Staff
Last Reviewed: February 26, 2026
Informed By:
Transplants.org, with participation from 23 leading U.S. transplant centers, led the largest comparative analysis of patient educational materials in transplant history. We recognize the participating centers who helped inform and inspire our direction with initial patient-centered educational content:
- Mayo Clinic (Co-Author)
- Vanderbilt University Medical Center (Co-Author)
- Johns Hopkins Hospital (Co-Author)
- UCLA Medical Center (Co-Author)
- UCSF Medical Center (Co-Author)
Transplants.org is an independent nonprofit organization and participation is not an endorsement by these organizations.